Speech Delay in Children: When to Act and How Therapies Help
ADHD Symptoms in Children — Myths vs Facts
Health Alliance
March 6, 2026
Child Developmental
Attention-deficit/hyperactivity disorder (ADHD) is the most talked-about disorder affecting children worldwide—and one of the most misunderstood neurodevelopmental conditions. Misconceptions about what ADHD looks like, what causes it, who it affects, and how it should be treated persist in homes, schools, and sometimes even clinical settings. This article analyzes common myths, provides facts, and explains clinical and practical nuances that parents, teachers, and caregivers need to know. Where relevant, I reference key public health and clinical guidance for accuracy.
What ADHD is (short, clear definition)
ADHD is a neurodevelopmental disorder characterized by patterns of inattention, hyperactivity, and impulsivity that are developmentally abnormal, disruptive, and occur in multiple settings (e.g., home and school). Symptoms typically begin in childhood (often before age 12) and can vary with age: younger children typically exhibit hyperactivity and impulsivity; as the need for sustained attention increases (e.g., at school), inattention symptoms become more pronounced.
The symptom clusters — what clinicians look for
Clinicians organize ADHD symptoms into two types:
- Inattention: Difficulty concentrating, frequent careless mistakes, feeling like you’re not listening, trouble following instructions, disorganization, losing things, and distraction.
- Hyperactivity–Impulsivity: Restlessness, inability to remain seated when expected, running or climbing in inappropriate situations, excessive talking, speaking out answers, or difficulty waiting for one’s turn.
Importantly, a diagnosis of ADHD is made when symptoms persist, appear excessive for the child’s developmental needs, and cause problems in two or more settings (e.g., home and school). The American Academy of Pediatrics recommends that primary care providers evaluate children ages 4-18 who are suspected of having ADHD and consider information from parents, teachers, and clinical observation. American Academy of Pediatrics
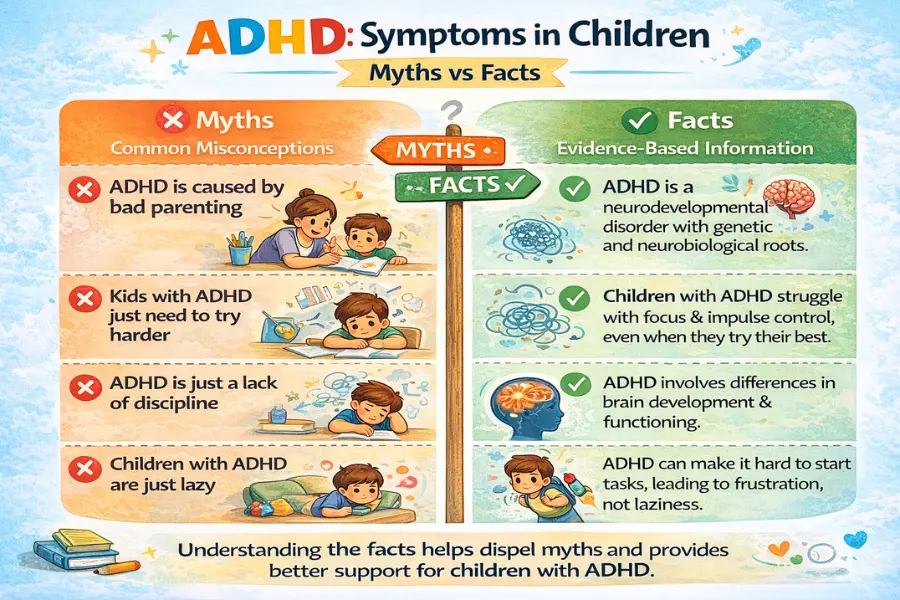
Myth 1 — “ADHD isn’t real; it’s just bad parenting or laziness”
Fact: ADHD is a validated neurodevelopmental disorder with biological and functional evidence.
This is a misconception that ignores one’s development. Decades of clinical research and modern neuroscience show that ADHD is linked to abnormal development and functioning in brain networks involved in attention, impulse control, and executive function (planning, working memory, cognitive flexibility). Although parenting style and classroom structure influence behavior and can exacerbate or mitigate symptoms, they do not cause ADHD. Blaming only parents ignores the neurobiological and genetic components of the disorder and delays appropriate treatment. Reputable organizations like the CDC and the National Pediatric Society recognize ADHD as a medical condition that requires assessment and specialized support.
Myth 2 — “All kids with ADHD are hyperactive”
Fact: There are different presentations; some children are primarily inattentive
ADHD has at least three common symptoms: mostly inattentive, mostly hyperactive-impulsive, and mixed. Children with mostly inattentive ADHD (formerly known as ADD) tend to be quiet and dreamy, have difficulty maintaining focus or organizing tasks, and are often overlooked because they don’t disrupt the classroom. This quiet nature can lead to missed diagnoses and later learning difficulties. Clinical guidance emphasizes evaluating behavior in different contexts to avoid overlooking these cases.
Myth 3 — “Kids will just ‘grow out of it’”
Fact: ADHD often persists into adolescence and adulthood, though symptoms can change
Some children experience less hyperactivity as they get older, and interventions or medications can mitigate the impairment—but many children continue to experience ADHD symptoms. Long-term research shows that many childhood ADHD symptoms persist into adolescence and adulthood, sometimes manifesting as problems with organization, time management, emotional regulation, and relationships. Early identification and evidence-based intervention reduce future risks (school failure, depression, substance abuse), so a “wait and see” approach when impairment is present is risky.
Myth 4 — “Sugar, food dyes, or ‘bad diet’ cause ADHD”
Fact: Diet can affect behavior but is not a primary cause of ADHD
Parents often hear that sugar or artificial colors cause hyperactivity. Scientific evidence does not support the idea that sugar is the primary cause of ADHD. Some children are sensitive to certain colors or additives, and dietary changes (such as eliminating artificial food dyes) may help some children. Overall, diet is important for overall health and may have a slight impact on behavior, sleep, and mood, but ADHD is not primarily a food-related disorder. If caregivers suspect a food sensitivity, a careful elimination trial under professional supervision is more responsible than general claims.
Myth 5 — “Medication is the only effective treatment — and it’s dangerous”
Fact: Medication can be very effective for many children, but it is one component of a broader treatment plan
Stimulant medications (such as methylphenidate and amphetamine formulations) and some non-stimulants are evidence-based treatments that can significantly reduce ADHD symptoms and improve functioning for many children. However, optimal care includes behavioral interventions (parent training, classroom support, behavioral therapy), educational support, and lifestyle interventions (sleep hygiene, exercise). For preschool-age children, behavioral parent training is usually most important before medication. Like all medications, ADHD medications have side effects and require monitoring; when prescribed and monitored by doctors, they are generally safe and effective. Resources from major clinical organizations provide age-appropriate advice.
Myth 6 — “Medication means you’re ‘fixing’ bad behavior”
Fact: Medication improves core symptoms which then allow learning of skills and better self-regulation
Medication is not a punishment or a moral judgment. For many children, reducing the core symptoms of inattention or agitation creates the biological bandwidth needed to learn behavioral strategies, complete tasks, and practice social skills. Medication and behavioral strategies have produced the best real-world results in numerous trials. The goal is to improve a child’s functioning and quality of life, not simply to “calm” the child down.
Comorbidities and differential diagnosis — why symptom overlap creates confusion
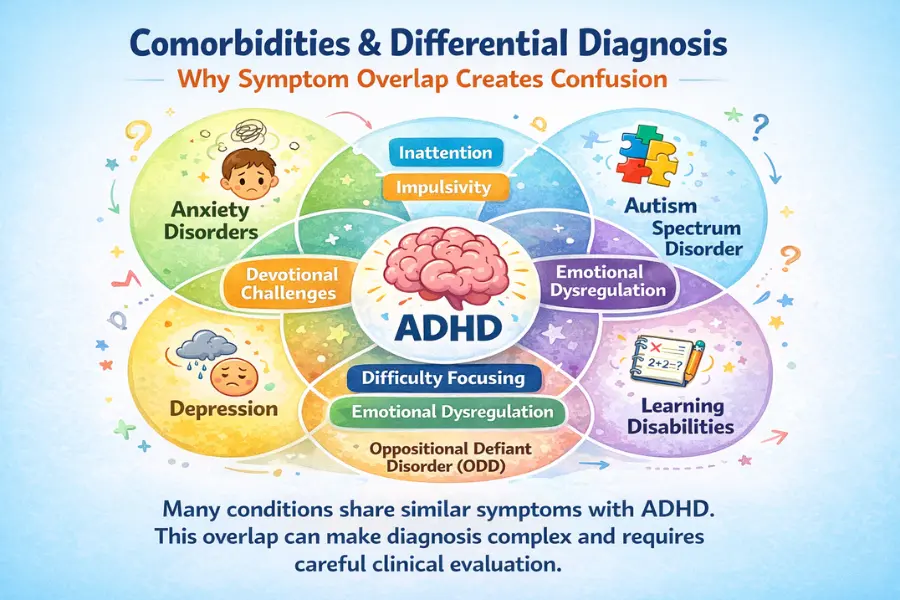
ADHD often co-occurs with other disorders: learning disorders, anxiety, depression, sleep disorders, oppositional defiant disorder, and autism spectrum disorders can occur simultaneously. Furthermore, sleep deprivation, sensory impairments, trauma, or hearing/vision problems can cause attention-like symptoms. Therefore, a thorough evaluation—collecting school and home reports, checking for learning difficulties and mood disorders, and considering medical and sleep problems—is essential before a definitive diagnosis can be made. Mislabeling an attention disorder without a thorough evaluation can lead to incorrect treatment.
Practical guidance for parents and teachers (evidence-informed)
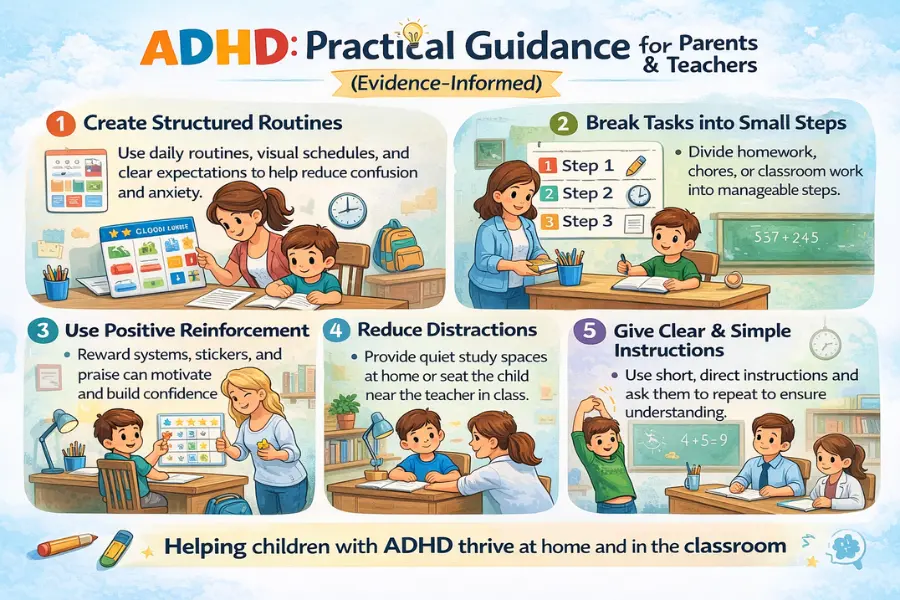
- Collect structured observations. Use teacher rating scales and systematic logs of when problems occur (task type, time of day, environment). Reliable information from multiple settings is crucial.
- Prioritize sleep and routines. Poor sleep can impair attention and behavior. Regular bedtimes, limited screen time before bed, and a consistent morning/evening routine can help.
- Behavioral strategies: Positive reinforcement, clear, concise instructions, breaking down tasks into steps, and immediate feedback improve adherence. For young children, parent training is crucial in behavior management.
- Educational supports: Individualized education programs (IEPs), 504 plans (in the U.S.), extra time for tests, seating near the teacher, and chunked assignments reduce academic failure. Coordination between home and school is essential.
- Consider professional evaluation when impairment is clear. If symptoms affect schoolwork, relationships with friends, or family life, a pediatrician, pediatric psychiatrist, or psychologist can evaluate and recommend evidence-based treatment.
Social and emotional aspects — the invisible load
In addition to the core symptoms, children with ADHD often experience shyness, low self-esteem, and social rejection. They may be labeled “lazy” or “naughty,” further exacerbating emotional harm. Therefore, interventions should focus on emotional literacy, peer skills, and fostering courage. Schools that adopt a strengths-based approach (recognizing abilities, assigning roles that match preferences, and explicitly teaching executive skills) improve both self-esteem and long-term outcomes.
When to worry: red flags that require urgent attention
Sedentary lifestyles, long screen hours, and poor ergonomics often result in chronic pain. Health Alliance offers specialized programs for professionals suffering from:
- Neck and shoulder pain
- Lower back pain
- Repetitive strain injuries
- Poor posture and spinal stress
Our ergonomic assessments and corrective programs make us a preferred physiotherapy clinic in Noida for corporate patients.
Final synthesis: a balanced view
ADHD is a real, diverse disorder. Misconceptions—from “it’s all sugar” to “kids will grow out of it” and “medications are always harmful”—lead to delays, stigma, and poor outcomes. The truth is that careful evaluation, a variety of interventions (behavioral, educational, sometimes medication-related), and family-school collaboration yield the best results. Identify the less obvious profiles (mostly inattentive), address comorbidities, and treat the child, not just create a checklist. The goal is practical: reduce impairments, build skills, and protect mental health.
For simple and up-to-date guidance, consult comprehensive resources like the Centers for Disease Control and Prevention, National Health Service (UK), American Academy of Pediatrics Clinical Guidelines, and specialty organizations that gather evidence and translate it into age-appropriate advice.
Short reading list / links (authoritative starting points)
- CDC — ADHD signs, symptoms and treatment.
- American Academy of Pediatrics — Clinical practice guideline for diagnosis & treatment.
- NHS (UK) — ADHD in children and young people.
- CHADD — myths and misunderstandings and caregiver resources.
- Mayo Clinic overview — symptoms and clinical features.